Chronic Obstructive Pulmonary Disease (COPD): Causes, Symptoms, Treatment, and Prevention
Introduction
Chronic Obstructive Pulmonary Disease, commonly known as COPD, is one of the leading causes of long-term illness and death worldwide. It is a progressive lung condition that makes breathing increasingly difficult over time. Despite being so common, many people don't realize they have COPD until the disease has already caused significant lung damage. This is because early symptoms are often mistaken for normal aging or a "smoker's cough."
The good news is that COPD is largely preventable, and with early diagnosis and proper management, people with COPD can live full, active lives. In this guide, we'll break down everything you need to know about COPD in simple, easy-to-understand language — from causes and symptoms to treatment options and prevention strategies.
What is COPD?
COPD stands for Chronic Obstructive Pulmonary Disease. It is an umbrella term used to describe a group of progressive lung diseases that cause airflow blockage and breathing-related problems. The two most common conditions that fall under COPD are:
Chronic bronchitis: Long-term inflammation of the airways (bronchial tubes) that leads to a persistent cough and excess mucus production.
Emphysema: Permanent damage to the air sacs (alveoli) in the lungs, which destroys their elasticity and reduces the surface area available for vital oxygen exchange.
Most people living with COPD have a combination of both conditions, in varying degrees of severity. COPD is a chronic (long-lasting) condition, meaning it does not go away, but its progression can be slowed significantly with the right care.
What Causes the Lung Damage?
While COPD itself is not an infectious disease, it is caused by long-term damage from inhaling lung irritants. The primary causes include:
Cigarette smoking: By far the leading cause, responsible for up to 85-90% of all COPD cases.
Long-term exposure to air pollutants: Including secondhand smoke, ambient outdoor air pollution, dust, chemical fumes, and vehicle emissions.
Occupational exposure: Industrial workers in mining, construction, textile, and manufacturing fields who regularly inhale dust and chemical irritants over many years.
Indoor air pollution: Cooking or heating with biomass fuels (wood, coal, or dung) in poorly ventilated spaces—a major cause of the condition in developing countries.
Genetic factors: A rare hereditary condition called Alpha-1 Antitrypsin Deficiency (AATD) can cause severe COPD even in individuals who have never smoked.
Frequent childhood respiratory infections: Severe lung infections during childhood can alter lung development and elevate the risk of developing COPD later in life.
How Respiratory Infections Spread
COPD itself is completely non-contagious—you cannot "catch" it from another person. However, individuals with damaged lungs are highly susceptible to respiratory infections like the flu, pneumonia, and common colds. These secondary infections spread via:
Airborne droplets generated during coughing or sneezing
Touching contaminated surfaces and transferring the pathogens to the eyes, nose, or mouth
Close physical contact with infected individuals
When a person with COPD catches a respiratory virus or bacteria, it can trigger a sudden, severe worsening of symptoms known as a COPD flare-up (or exacerbation), which frequently requires emergency medical care or hospitalization.
Who is at Higher Risk?
The likelihood of developing chronic airflow limitation increases with specific demographic and lifestyle factors:
Current and former smokers: The risk scales directly with the number of years and packs smoked per day.
People over 40 years old: Due to the gradual accumulation of lung exposure, symptoms typically manifest in middle age or later.
Individuals with a family history of COPD: Genetic predispositions can lower lung defense mechanisms.
Asthma patients: Long-term, poorly controlled asthma significantly compounds the risk of fixed airway obstruction.
Industrial workers: Anyone exposed to chemical vapors, fumes, and organic or inorganic dust in the workplace.
Highly polluted environments: Individuals living or working in regions with dense industrial emissions or heavy traffic.
Signs and Symptoms
COPD symptoms typically develop at a slow pace and progress in severity over the years. Common signs include:
A persistent, chronic cough, often accompanied by clear, white, yellow, or greenish mucus (sputum)
Progressive shortness of breath (dyspnea), particularly during physical activities like walking or climbing stairs
Frequent wheezing or a distinct whistling sound while breathing
Chronic chest tightness or discomfort
Increased vulnerability to seasonal chest infections
Generalized fatigue and lack of physical energy
Unintended weight loss (frequently observed in advanced stages of emphysema)
Swelling in the ankles, feet, or legs due to strain on the heart's circulatory path
When to Seek Medical Help
It is critical to schedule an evaluation with a physician if you experience a persistent cough lasting more than a few weeks, progressive shortness of breath that limits daily tasks, or frequent chest infections.
Emergency Warning Signs: If you or a loved one experience sudden, severe breathlessness, bluish lips or fingernail beds (cyanosis), confusion, slurred speech, or a rapid heart rate, seek emergency medical attention immediately. These are life-threatening signs of respiratory failure.
For professional, targeted care regarding ongoing breathing issues, consulting a Pulmonologist is strongly recommended, as they specialize in diagnosing and managing complex lung conditions like COPD.
Diagnosis and Testing
Accurately diagnosing COPD involves a multi-step clinical assessment to rule out overlapping conditions like heart failure or asthma:
Medical history and physical examination: Evaluating smoking habits, environmental exposures, and listening to lung sounds.
Spirometry: The primary diagnostic test for COPD. It requires blowing into a machine that measures how much air your lungs can hold and how fast you can exhale it.
Chest X-ray or CT scan: Imaging tests used to visualize lung tissue structural changes (like emphysema) and rule out other diseases like lung cancer.
Arterial Blood Gas (ABG) test: A blood sample drawn from an artery to measure precise levels of oxygen and carbon dioxide.
Alpha-1 Antitrypsin testing: A simple blood test recommended for younger individuals who show early symptoms of COPD without a history of smoking.
Treatment and Management
While there is no permanent cure to reverse lung damage, clinical treatments aim to ease breathing, prevent flare-ups, and preserve long-term quality of life.
Bronchodilators: Inhaled medications that relax muscle bands around the airways to open them up.
Inhaled Corticosteroids: Medications that reduce chronic airway inflammation, prescribed to lower the frequency of severe exacerbations.
Combination Inhalers: Devices delivering both a bronchodilator and an anti-inflammatory steroid simultaneously.
Oxygen Therapy: Supplemental oxygen delivered via nasal prongs or masks for patients with severe resting hypoxemia (low blood oxygen).
Pulmonary Rehabilitation: A specialized, comprehensive program combining monitored exercise training, nutritional counseling, and breathing strategies.
Vaccinations: Crucial preventative healthcare to insulate damaged lungs from preventable infections.
Surgical Options: For end-stage cases, procedures such as lung volume reduction surgery (LVRS) or a lung transplant may be evaluated. Diagnostic procedures like an Endoscopy may be used to look inside the lungs during pre-surgical evaluations.
Lifestyle adjustments—especially absolute smoking cessation, eating nutrient-rich foods, staying physically active within safe limits, and staying clear of secondhand smoke—are the pillars of managing this condition.
Recovery and Management Timeline
Because COPD is a permanent, progressive chronic disease, it does not follow a typical acute recovery timeline. Instead, milestone improvements focus on disease stability:
Timeline | Anticipated Clinical Milestone |
Immediate (Days) | Quitting smoking stops the accelerated drop in lung function and helps clear carbon monoxide from the blood. |
2–4 Weeks | Initialization of proper bronchodilator therapy typically yields a noticeable reduction in daily breathlessness and coughing. |
6–12 Weeks | Completion of a structural Pulmonary Rehabilitation program significantly increases physical stamina and reduces fatigue. |
1–2 Weeks | Most acute flare-ups (exacerbations), when treated promptly with antibiotics or steroids, resolve back to baseline function. |
Prevention Strategies
Protecting your lungs early in life is the most effective approach to preventing irreversible airway disease:
Avoid tobacco use: Never pick up smoking, and take active steps to quit immediately if you currently smoke.
Minimize secondhand exposure: Stay clear of areas where tobacco smoke accumulates.
Use occupational safety gear: Wear certified respirators and masks if your work exposes you to airborne dust, masonry particles, or chemical gases.
Ventilate cooking spaces: Ensure proper exhaust fans or chimneys are operational, especially if cooking with wood or biomass fuels inside.
Keep moving: Regular aerobic exercise helps maximize chest wall mechanics and systemic oxygen utilization.
Track outdoor air quality: Stay indoors or wear protective masks on days when the local air quality index indicates dangerous pollutant levels.
Preventive Vaccines
While vaccines do not treat the damaged lung structures directly, staying up to date on immunizations prevents severe, potentially fatal flare-ups:
Annual Influenza (Flu) Vaccine: Helps prevent seasonal flu strains that heavily irritate inflamed bronchial tubes.
Pneumococcal Vaccine: Provides protection against specific bacterial pathogens responsible for pneumonia, meningitis, and bloodstream infections.
COVID-19 Vaccine: Highly recommended to prevent severe respiratory complications associated with coronavirus variants.
Common Myths vs. Facts
Myth: COPD only affects heavy smokers.
Fact: While smoking is the predominant cause, up to 15-20% of COPD patients are lifelong non-smokers who developed the condition from air pollution, genetics, or toxic workplace dust.
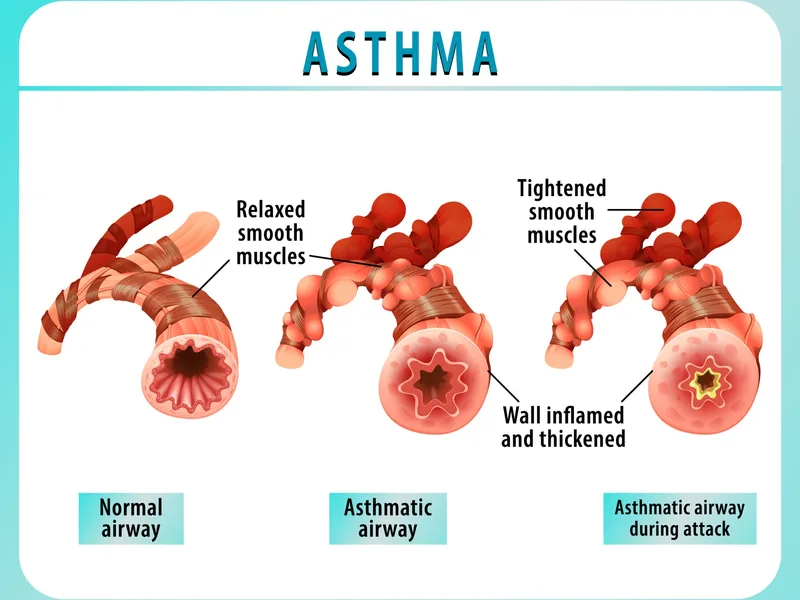
Myth: COPD is exactly the same as asthma.
Fact: Both conditions involve airway obstruction, but asthma is a highly reversible allergic airway response, whereas COPD involves fixed, progressive, and permanent damage to airways and air sacs.
Myth: If you quit smoking, your COPD will vanish completely.
Myth: Inhalers are only useful when having a breathing crisis.
Complications
Unmanaged or severely progressive COPD can give rise to a range of systemic medical complications:
Frequent Respiratory Infections: High vulnerability to severe bouts of acute bronchitis or bacterial pneumonia.
Cardiovascular Diseases: Increased structural stress on the right side of the heart, expanding the risk of heart attacks and heart failure. A qualified Cardiologist is frequently called upon to monitor and manage these intertwined cardiopulmonary risks.
Pulmonary Hypertension: Elevated, dangerous blood pressure levels specifically localized within the arteries serving the lungs.
Lung Cancer: Chronic cellular inflammation from long-term smoking significantly increases the statistical incidence of malignant lung tumors.
Mental Health Impact: Managing a chronic disease that affects breathing commonly triggers secondary anxiety, panic disorders, and depression.
Acute Respiratory Failure: A state where the lungs can no longer clear out sufficient carbon dioxide or absorb enough atmospheric oxygen to sustain vital organs.
Frequently Asked Questions (FAQs)
1. What is the primary cause of COPD?
Cigarette smoking is the single biggest cause of COPD globally, accounting for up to 90% of documented diagnoses.
2. Can the lung damage from COPD be fully cured?
No, the architectural damage to the alveoli and bronchial walls is irreversible. However, custom medical regimens can significantly reduce daily symptoms and preserve your quality of life.
3. What is the key difference between COPD and emphysema?
Emphysema is not a separate disease; rather, it is a component of COPD. Emphysema refers specifically to the structural breakdown of the microscopic lung air sacs, while COPD is the overall disease term.
4. What are the earliest warning signs of developing COPD?
An ongoing, daily cough that produces mucus, frequent throat clearing, and subtle breathlessness during standard household tasks are the primary early indicators.
5. Is it possible for a lifelong non-smoker to get COPD?
Yes. Long-term exposure to heavy industrial dust, chemical fumes, severe outdoor smog, or inheriting the Alpha-1 Antitrypsin Deficiency gene can cause COPD in non-smokers.
6. What diagnostic test definitively confirms COPD?
Spirometry is the definitive diagnostic gold standard. It objectively evaluates how well your lungs exhale air against baseline norms.
7. What is the overall life expectancy after a COPD diagnosis?
Life expectancy varies broadly based on how early the disease is detected, your adherence to medical management, and whether you continue to smoke. Many people live active lives for decades after diagnosis.
8. Should I avoid exercising if I have COPD?
No, avoiding movement can actually cause your muscles to weaken, making breathlessness worse over time. Safe, moderate physical activities and structured pulmonary rehabilitation are highly beneficial.
9. Is COPD contagious to family members?
No, COPD is entirely a chronic environmental and genetic condition; it cannot be transmitted from person to person. However, seasonal viruses that cause flare-ups can be passed along.
10. Are there specific foods I should limit with COPD?
It is wise to limit heavily salted foods, processed meats, and large portions of gas-producing foods (like carbonated beverages or beans). Bloating pushes the diaphragm upward, making it harder for your lungs to expand.
11. Why does COPD affect emotional and mental health?
The ongoing feeling of breathlessness can trigger a biological panic response, leading to chronic anxiety. The restriction of daily physical activities can also contribute to feelings of depression.
12. How frequently should I follow up with my physician?
Most individuals stable on their medications should see their primary provider or pulmonologist every 3 to 6 months for spirometry checks and regular prescription reviews.
13. How do doctors distinguish between asthma and COPD?
Asthma often begins in childhood, is triggered by allergies, and lung function can return to normal between episodes. COPD typically manifests after age 40, is tied to smoking/pollution, and causes permanent airway blockage.
14. Does having COPD make me more susceptible to lung cancer?
Yes, the chronic tissue damage and underlying inflammation, paired with shared risk factors like smoking, result in a significantly higher risk of developing lung cancer.
15. Where can I find specialized, comprehensive treatment for advanced COPD?
Seeking care at designated Multispecialty Hospitals in Kolkata provides immediate access to expert pulmonologists, advanced diagnostic imaging, full-scale pulmonary rehabilitation infrastructure, and emergency respiratory care.
Conclusion
COPD is a serious, lifelong condition, but it responds well to structured medical care and positive lifestyle changes. Early medical intervention can help preserve lung function and keep you active. If you or someone close to you is dealing with an ongoing cough or frequent shortness of breath, do not wait for the symptoms to worsen—reach out to a healthcare professional right away. Taking action early is the most effective way to protect your long-term lung health.