Free Helpline
We are here to assist you.
Health Advisor
+91-8877772277Available 7 days a week
10:00 AM – 6:00 PM to support you with urgent concerns and guide you toward the right care.
We are here to assist you.
Health Advisor
+91-8877772277Available 7 days a week
10:00 AM – 6:00 PM to support you with urgent concerns and guide you toward the right care.
Explore 'Pure O', a form of OCD where compulsions are mental, not physical. Learn about its symptoms, diagnosis, and effective treatments like ERP and CBT.

What is Pure O? The term "Pure O" is often used to describe a form of Obsessive-Compulsive Disorder (OCD) where the compulsions are primarily mental rather than physical. It's important to understand that "Pure O" is not a formal clinical diagnosis in itself, but rather a way to describe a specific experience within the broader spectrum of OCD. For individuals experiencing Pure O, the distress caused by intrusive thoughts (obsessions) is managed through internal mental rituals instead of visible, repetitive actions like handwashing or excessive cleaning. While the name might suggest an absence of compulsions, this is a misnomer. People with Pure O do engage in compulsions, but these are often hidden and occur within their minds. This can make it challenging for both the individual and those around them to recognize the presence of OCD, as the outward signs are not as apparent. Obsessions and Compulsions in OCD OCD is characterized by two core components: obsessions and compulsions. Obsessions: These are unwanted, intrusive, and persistent thoughts, images, or urges that cause significant distress and anxiety. They are difficult to control or ignore and can be about a wide range of topics. Compulsions: These are repetitive behaviors or mental acts that a person feels driven to perform in response to an obsession. The goal of a compulsion is typically to reduce the anxiety caused by the obsession or to prevent a feared outcome. The Difference in Pure O The key distinction in Pure O lies in the nature of the compulsions. While individuals with classic OCD might exhibit physical compulsions like excessive washing, checking locks, or arranging objects symmetrically, those with Pure O predominantly engage in mental compulsions. These can include: Mental Review: Repeatedly going over past events or conversations in one's mind to ensure nothing was done wrong or offensive. Reassurance Seeking: Mentally asking oneself or others for reassurance that a feared outcome will not happen. Mental Neutralization: Performing mental rituals, such as repeating a specific word or phrase (mantra), praying silently, or visualizing positive images to counteract or cancel out an obsessive thought. Rumination: Getting stuck in thought loops, endlessly analyzing situations or feelings without reaching a resolution. Because these compulsions are internal, they can be exhausting and time-consuming, even though they are not visible to others. The individual may appear outwardly normal, but internally they are battling intense anxiety and engaging in significant mental effort to cope. Common Themes in Pure O Pure O obsessions can revolve around any theme, just like other forms of OCD. Some common themes include: Harm OCD: Intrusive thoughts or images of harming oneself or others, often accompanied by intense guilt and fear of acting on these thoughts. Relationship OCD (ROCD): Doubts and anxieties about one's romantic relationships, partners, or feelings for them. Sexual Orientation OCD: Persistent intrusive thoughts and doubts about one's sexual orientation. Scrupulosity OCD: Obsessions related to religious or moral beliefs, often involving fears of blasphemy or sinning. Existential OCD: Deep philosophical worries about the meaning of life, death, or reality. Mental Health OCD: Fear of having a mental illness, such as schizophrenia or bipolar disorder, leading to constant self-monitoring and reassurance seeking. It's crucial to remember that having these intrusive thoughts does not mean a person wants them to happen or will act on them. The distress and fear associated with these thoughts are hallmarks of OCD. Diagnosis of OCD (Including Pure O) A formal diagnosis of OCD is made by a qualified mental health professional based on specific criteria. The term "Pure O" might be used to describe the presentation, but the diagnosis remains OCD. The diagnostic criteria generally include: Presence of Obsessions and/or Compulsions: The individual experiences recurrent, persistent, and intrusive thoughts, urges, or images (obsessions) and/or engages in repetitive behaviors or mental acts (compulsions). Time-Consuming Symptoms: The obsessions and compulsions are significantly time-consuming (e.g., taking up more than an hour per day) and cause marked distress or impairment in social, occupational, or other important areas of functioning. Exclusion of Other Conditions: The symptoms are not attributable to the physiological effects of a substance (e.g., a drug of abuse, a medication) or another medical condition. A mental health professional will conduct a thorough assessment, which may include interviews, questionnaires, and discussions about the nature and frequency of thoughts and behaviors. Treatment for Pure O The treatment for Pure O is largely the same as for other forms of OCD, focusing on managing obsessions and reducing the impact of compulsions. The most effective treatments include: Exposure and Response Prevention (ERP): This is considered the gold standard treatment for OCD. It involves gradually exposing the individual to their feared thoughts or situations (exposure) and then preventing them from engaging in their usual compulsive behaviors (response prevention). For Pure O, this might involve learning to tolerate intrusive thoughts without resorting to mental rituals. Cognitive Behavioral Therapy (CBT): CBT helps individuals identify and challenge distorted thought patterns associated with obsessions. It teaches coping strategies to manage anxiety and reduce the believability of intrusive thoughts. Medication: Selective Serotonin Reuptake Inhibitors (SSRIs) are often prescribed to help manage OCD symptoms by regulating serotonin levels in the brain. These medications can reduce the intensity and frequency of obsessions and compulsions. Therapy is crucial for developing skills to manage the internal struggles of Pure O. It empowers individuals to regain control over their thoughts and reduce the distress they cause. When to Consult a
In summary, timely diagnosis, evidence-based treatment, and prevention-focused care improve long-term health outcomes.
High-functioning anxiety is not a clinical diagnosis — but it describes a real and pervasive experience. People with high-functioning anxiety appear capable and successful on the outside while experiencing persistent internal distress. Recognising the pattern is the first step to changing it.
April 14, 2026
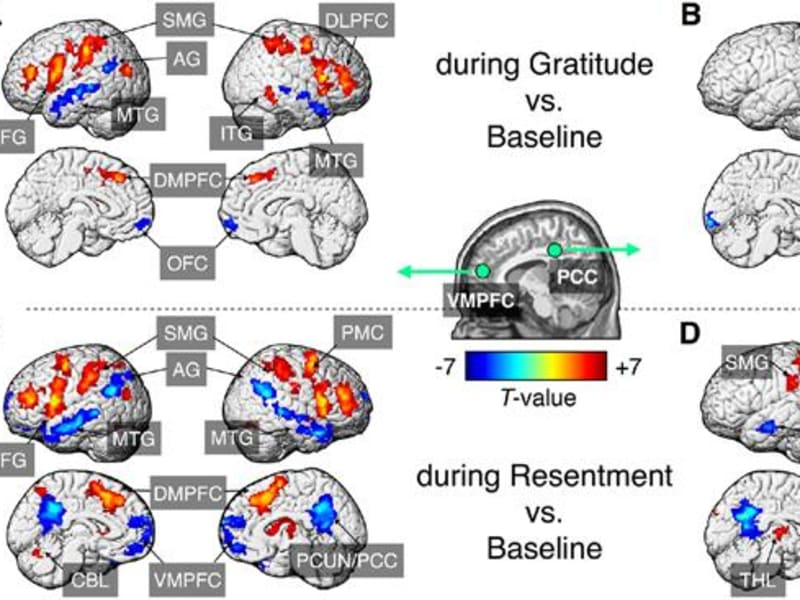
Gratitude practices have moved from self-help cliché to serious neuroscience. Brain imaging studies, randomised trials, and neurochemical research now reveal how consistent gratitude practice physically alters neural circuits linked to mood, anxiety, and social connection.
April 14, 2026
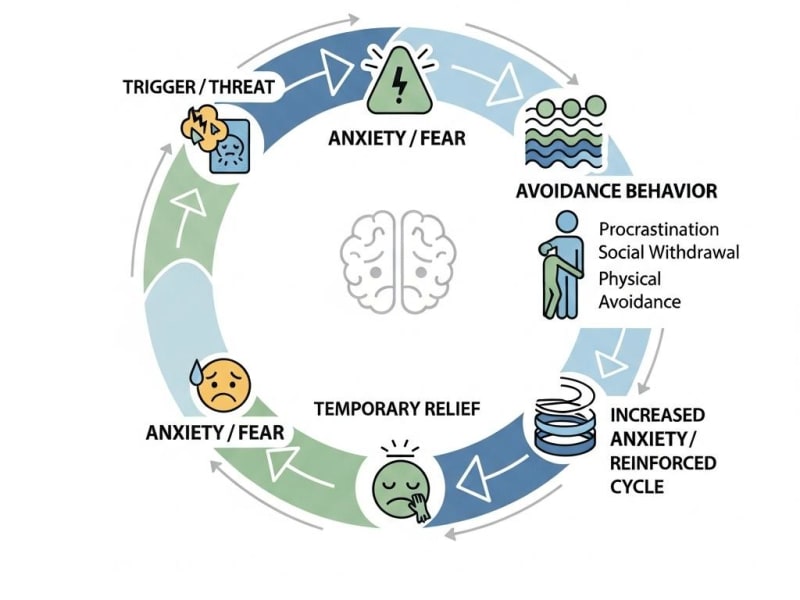
Avoiding anxiety-provoking situations feels like relief — but it's actually the mechanism that makes anxiety chronic. Understanding and interrupting the anxiety-avoidance cycle is the foundation of every effective psychological treatment for anxiety disorders.
April 14, 2026